
Having a loved one admitted to the Intensive Care Unit (ICU) and put on a ventilator can be frightening. The view of tubes, machines, and monitors can create panic, confusion, and lots of questions — the most prevalent question being: “Will they ever come off the ventilator?”
As a critical care physician, I’ve seen that misunderstanding about ventilators leads to unnecessary fear. This blog aims to clear the air by busting common myths, sharing the facts, and helping families understand why ventilators are often life-saving tools — not life-ending ones.
What Is a Ventilator and How Does It Work?
A ventilator, or mechanical ventilator, is a device that assists or takes over breathing when an individual’s lungs are not working properly.
It does this by:
- Forcing oxygenated air into the lungs
- Assisting in the removal of carbon dioxide
- Providing the lungs with time to rest and recover
Ventilators are employed in emergencies, surgery, or serious illnesses such as pneumonia, sepsis, trauma, or COVID-19.
Common Myths About Ventilators — Debunked!
Myth 1: Being on a ventilator means the patient is about to die.
Fact: Ventilators are used to save lives. Many patients recover fully and come off the ventilator once their lungs improve. In some cases, patients are put on ventilators temporarily during surgery or for reversible conditions.
Myth 2: Once a person is on a ventilator, they’ll never come off.
Fact: We slowly wean most patients off the ventilator. It lasts for as long as the underlying condition, age, and health require. We watch every patient very closely and take the ventilator out as soon as it’s safe to do so.
Myth 3: Ventilators hurt or cause suffering.
Fact: Ventilator patients are most often sedated, and we take extra care to make them comfortable. In case the patient is awake, we apply measures to cause them minimal discomfort and anxiety.
Myth 4: Families must “not permit” the use of ventilators if the situation is critical.
Fact: Withholding or not initiating ventilator care is a serious choice. When there is curable illness, withholding ventilation too early may decrease chances of survival. We always engage families in open discussion regarding prognosis and care goals.
When is a Ventilator Indicated?
Ventilators are usually indicated when:
- Oxygen levels fall to dangerously low levels
- Carbon dioxide accumulates
- The patient is comatose or unconscious
- Severe infection (e.g., sepsis or COVID-19 pneumonia)
- There’s respiratory failure from trauma or heart failure
What Families Need to Know When a Loved One Is Ventilated
1. It’s Not a Death Sentence
Numerous ICU survivors were once ventilator patients — and left the hospital under their own steam after successful therapy.
2. Ask About the Underlying Cause
Knowing why ventilation is necessary can help anticipate how long it will be needed. Ask the ICU team:
- What condition led to this?
- Is it reversible?
- What is the short-term goal?
3. Get to Know the Ventilator Settings
Ventilators can offer:
- Full support (machine works for them)
- Partial support (they breathe with assistance)
- Weaning trials (practicing readiness to breathe without help)
- We gradually withdraw support as the patient gets better.
4. Stay Updated — But Be Patient
Recovery of the lungs does take time. Improvement won’t always be evident from day to day. But many subtle improvements accumulate. Dr. Amit Choudhary’s ICU team offers daily feedback and facilitates family decision-making in a clear and compassionate way.
What Are the Risks of Being on a Ventilator?
Although ventilators save lives, they do pose some risks:
- Ventilator-Associated Pneumonia (VAP)
- Lung damage from high pressure (barotrauma)
- Delirium or confusion from sedation
- Muscle weakness
Our staff reduces these hazards with lung-protective measures, frequent suctioning, and sedation management guidelines.
Can Patients Breathe Without the Tube Later?
Yes. The procedure is called weaning:
- The patient breathes more on his or her own.
- Ventilator settings are decreased.
- If breathing continues to be stable, the tube is taken out (extubation).
Some patients might require a tracheostomy (a neck tube) if they need long-term assistance — but even this is temporary.
Ventilator Care in Dr. Amit Choudhary’s ICU
Our ICU integrates innovative ventilation methods with:
- Patient and family education
- Minimal sedation policies
- Weaning assessment on a daily basis
- Emotional support to caregivers
- Open communication regarding prognosis
Key Takeaways
- A ventilator is a breathing aid not a death warrant.
- Most patients recover and are successfully weaned from the ventilator.
- Families are encouraged to question and be informed.
- Risks do occur, but are safely controlled in a contemporary ICU environment.
Recent Posts
-
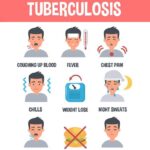 Understanding Tuberculosis: Symptoms, Diagnosis, and Treatment Options
Understanding Tuberculosis: Symptoms, Diagnosis, and Treatment Options -
 Diabetes and Its Emergencies: Symptoms, Risks & Quick Action
Diabetes and Its Emergencies: Symptoms, Risks & Quick Action -
 Sepsis Management: Critical Care Strategies that Save Lives
Sepsis Management: Critical Care Strategies that Save Lives -
 Understanding ICU Alarms: What Families Should Know
Understanding ICU Alarms: What Families Should Know -
 Why Follow-up OPD Consultations Are Essential Following an ICU Stay
Why Follow-up OPD Consultations Are Essential Following an ICU Stay